

Artificial Sweeteners: Insulin Neutral or Metabolically Misleading?
Artificial sweeteners are often promoted as metabolically neutral alternatives to sugar. However, insulin regulation involves more than calories alone. Research suggests that some artificial sweeteners may influence insulin signaling, appetite regulation, gut microbiota, and metabolic outcomes – sometimes without obvious changes in blood glucose. Understanding these mechanisms is essential for evaluating whether “sugar-free” truly supports metabolic health.¹,²
Artificial Sweeteners: A Metabolic Signal, Not Just a Flavor
Artificial sweeteners (commonly referred to as non-nutritive sweeteners) include compounds such as aspartame, sucralose, saccharin, and acesulfame-K. While these sweeteners contribute little to no energy, sweetness itself is a biological signal. Sweet taste receptors evolved to anticipate carbohydrate intake and initiate metabolic preparation.³
Importantly, these receptors are expressed not only on the tongue but also throughout the gastrointestinal tract, where they may influence incretin hormones and insulin secretion.⁴
Do Artificial Sweeteners Stimulate Insulin?
Some studies suggest artificial sweeteners can trigger a cephalic phase insulin response (CPIR), which is a small, anticipatory insulin release initiated by sweet taste alone.⁵ While typically modest, repeated stimulation may be relevant in individuals with insulin resistance.
Additionally, activation of intestinal sweet taste receptors may influence incretin hormones such as GLP-1, indirectly affecting insulin dynamics.⁶
Human Trial Evidence: Mixed but Instructive
Short-term randomized trials often show no acute rise in blood glucose or insulin when artificial sweeteners are consumed alone.⁷ This has contributed to the belief that they are metabolically inert.
However, longer-term observational studies consistently associate habitual artificial sweetener consumption with:
- Increased risk of type 2 diabetes
- Higher prevalence of metabolic syndrome
- Impaired insulin sensitivity⁸,⁹
While observational data cannot establish causality, these findings suggest that metabolic effects may emerge over time and in specific populations.
The Gut Microbiome Connection
Artificial sweeteners may alter gut microbial composition, potentially influencing glucose tolerance and insulin sensitivity. Animal models and early human data suggest that changes in microbial metabolites and inflammation may mediate these effects.¹⁰,¹¹
Because the gut microbiome plays a central role in metabolic regulation, even subtle disruptions may have downstream consequences for insulin signaling.
Sweetness Without Calories: A Predictive Mismatch
From a metabolic perspective, sweetness without energy creates a sensory-metabolic mismatch. The nervous system predicts incoming glucose, but when it fails to arrive, compensatory mechanisms may increase appetite, cravings, or subsequent energy intake.¹²,¹³
This mismatch may partially explain why artificial sweeteners do not consistently improve long-term metabolic outcomes despite reducing sugar intake.

Are Artificial Sweeteners Helpful or Harmful?
Potential Benefits
- Reduce added sugar intake
- Do not raise blood glucose acutely
- May support short-term dietary transitions
Potential Downsides
- Possible insulin signaling through sensory pathways
- Gut microbiome disruption
- Reinforcement of sweet taste dependence
- Associations with insulin resistance in long-term studies⁸,⁹
Practical, Metabolism-First Guidance
- Minimize habitual sweetness exposure
- Use sweeteners strategically, not routinely
- Prioritize whole foods with predictable metabolic responses
- Monitor individual responses, especially in insulin-resistant states
Sweetener Summary
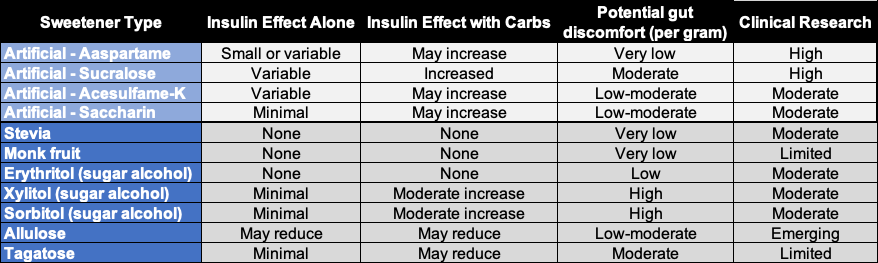
How to Interpret This Chart (Important Context)
- Insulin response is context-dependent: A sweetener that appears “neutral” on its own may amplify insulin signaling when combined with carbohydrates, especially in insulin-resistant individuals.
- Sweet taste alone can still signal insulin: Some artificial sweeteners can stimulate a cephalic phase insulin response, even without calories—this effect is small but potentially relevant over time.
- Liver effects matter: Sweeteners high in fructose may not spike insulin immediately but can increase liver fat, worsening insulin resistance downstream.
- Individual responses vary: People with insulin resistance, metabolic syndrome, or diabetes may experience greater insulin responses than metabolically healthy individuals.
Conclusion
Artificial sweeteners are not metabolically invisible. While they may reduce sugar intake and blunt immediate glucose spikes, they can interact with insulin signaling, gut physiology, and appetite regulation in ways that matter—particularly over time. A metabolism-first approach prioritizes reducing sweetness dependence altogether rather than relying on increasingly engineered substitutes.
FAQs
Do artificial sweeteners raise insulin?
Some may stimulate insulin indirectly via cephalic or gut-mediated mechanisms, though responses vary.
Are they safe for people with diabetes?
They may help reduce short-term glucose excursions, but long-term metabolic effects remain uncertain and individualized.
Do they affect gut health?
Certain artificial sweeteners appear to alter gut microbiota, which may influence insulin sensitivity.
Are all artificial sweeteners the same?
No. Different compounds have distinct effects on insulin signaling, gut tolerance, and metabolic outcomes.











 30 Day Money Back Guarantee
30 Day Money Back Guarantee